Hey everyone! Today I want to talk about a topic that is close to my heart – osteonecrosis. Living with this rare condition can be really challenging, both physically and mentally. Osteonecrosis occurs when there is a lack of blood supply to the bone and joint, which can eventually lead to the collapse of the bone and the need for a joint replacement. It’s a tough journey, but remember, you’re not alone.
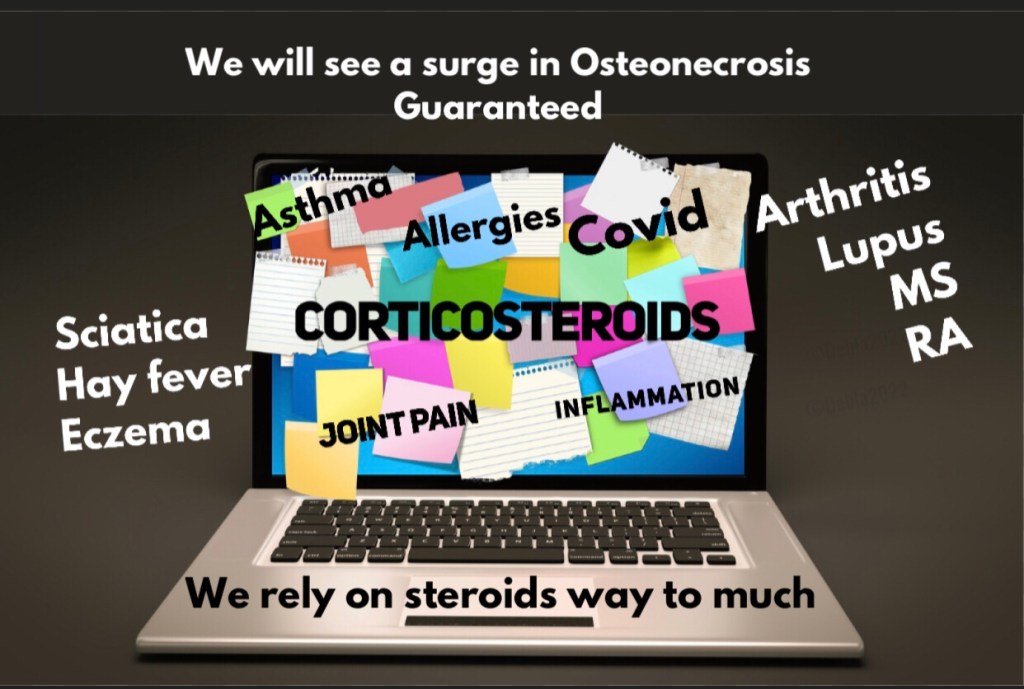
There are various underlying causes for osteonecrosis, including trauma to the bone or joint, blood clotting disorders, autoimmune conditions, cancer treatments like radiation and chemotherapy, as well as certain diseases like vasculitis, lupus, HIV, and sickle cell anemia. Lifestyle factors such as smoking and excessive drinking can also contribute to the development of osteonecrosis. Additionally, the chronic use of corticosteroids is a known cause for many individuals.
However, it’s crucial to note that not everyone who experiences these factors will develop osteonecrosis. Each person’s journey with this condition is unique, and it’s important not to blame ourselves or feel guilty for something that may be beyond our control.
But here’s the thing – we need better treatment options for osteonecrosis. Having access to alternative medications like platelet-rich plasma (PRP) therapy can make a significant difference in managing this condition and potentially preventing the need for joint replacements. PRP therapy involves using a concentrated form of a patient’s own blood to promote healing and regeneration in the affected area.
Unfortunately, insurance companies often don’t cover PRP therapy or other alternative treatments for osteonecrosis. This makes it challenging for individuals to explore all available options to manage their condition effectively. We need to raise awareness about the importance of these treatments and advocate for insurance coverage, ensuring that everyone has access to the best possible care.
So, let’s come together and spread awareness about osteonecrosis. Share your experiences and knowledge, support one another, and join the fight for better treatment options. Together, we can make a difference in the lives of those living with this condition. Don’t forget to use the hashtags #OsteonecrosisAwareness and #JointHealthMatters to amplify our message.
Remember, everyone’s journey is unique, but together we can make a difference. Let’s continue to spread awareness and support one another in this fight against osteonecrosis. Stay strong, warriors! 💪🙌

The Guardian
I’m excited to share with you one of the new logo designs for Osteonecrosis awareness! Introducing “The Guardian” – a symbol of strength, protection, and unity in the fight against this rare condition.
The logo features a bold and powerful image of a guardian angel with outstretched wings, symbolizing the support and protection we offer to those affected by osteonecrosis. The angel is seen holding a bone, representing the importance of bone health and the need to raise awareness about this condition.
The color palette chosen for the logo reflects the resilience and determination of individuals living with osteonecrosis. Shades of blue and purple evoke a sense of calmness, hope, and empowerment, while the green is for life and the touch of gold -white adds a touch of elegance and sophistication.
The Guardian logo aims to capture attention and spark curiosity, encouraging individuals to learn more about osteonecrosis and become advocates for better treatment options and insurance coverage. By using this logo, we are creating a unified and recognizable symbol that can be shared across social media platforms, websites, and events, creating a sense of community and solidarity.
As an influencer, it’s essential for me to use my platform to spread awareness and support those affected by osteonecrosis. I encourage you all to join me in using the hashtag #GuardianOfBoneHealth when sharing posts related to this condition and the new logo. Let’s come together and make a positive impact in the lives of individuals battling osteonecrosis.
Stay strong and keep fighting, warriors! 💙💜💚
Logo 2 The Multi-Phoenix
Also is
The phoenix is a powerful symbol of transformation and resilience, which aligns perfectly with the journey of those living with osteonecrosis. By incorporating the phoenix logo into our social media posts, we can further emphasize the strength and determination of individuals battling this condition.
Let’s use the hashtag #RisingStrong to accompany posts featuring the phoenix logo. Together, we can inspire hope and encourage others to rise above challenges and embrace their own inner strength.
If you’re interested in using the phoenix logo on your social media platforms, feel free to reach out to me for the high-resolution image. Let’s continue raising awareness and supporting one another in this journey of resilience.
Stay powerful, warriors! 🔥💪