
With online scams reaching epidemic proportions, Instagram is just the latest channel for fraudsters to make a quick buck. With over 1 billion active…
Instagram Scammers Stealing your info or Hackers taking your account.

Avascular Necrosis-Osteonecrosis Education and Resources
Avascular Necrosis-Osteonecrosis Education and Resources
With online scams reaching epidemic proportions, Instagram is just the latest channel for fraudsters to make a quick buck. With over 1 billion active…
Instagram Scammers Stealing your info or Hackers taking your account.
This is a really good app, it’s new released by the arthritis foundation just a couple weeks ago.
It’s a great way to connect with others that understand what it’s like to live with pain.
It provides tips to help ease the stress and anxiety that come with chronic pain.
Discusses various treatments from diet to meditation, to acupuncture to prp and stem cell injections to joint replacement .
The app tries to help those living in pain have options to have a better quality of life. It helps track your pain so you can discuss this with your doctor or surgeon.
It also gives you ways to register to get connected with National and at Some point Local connect groups in your area . All this is free. Ypu can even link to the podcast.
I am the Facilitator for the Boardman Ohio LIVE Yes Connect. I try to provide support, and patient education via information as well as guest speakers as well as group interaction.
Right now we are on zoom, but will be at some point back face to face as well as remain on zoom also. I think zoom is good because you can attend right from your hone or work or pulled over in your can.
That’s why I volunteer for the Arthritis Foundation, they provide so much to so many.
Give it a try…. one of the best apps I have.
If you use it. Use the same email as your arthritis.org email for Live Yes Connect. That way you can be up to date and linked to all great things the AF has to offer in one easy app.
Wishing you all a pain free day
Deb

Osteonecrosis is a well-recognized complication associated with organ transplantation.
It is a pathological condition characterized by the death of the cellular constituents of bone and marrow. The process of aseptic bone necrosis is associated with glucocorticoid use, and the mechanism by which glucocorticoids initiate the pathologic process has recently been elucidated.
Rates are particularly high in patients with systemic lupus erythematosus. The incidence of osteonecrosis also increases in patients on dialysis.
The exact prevalence of osteonecrosis after organ transplantation is, however, difficult to assess as many cases are clinically silent.
The most common symptom of osteonecrosis is hip pain that is usually deep in nature, localized to the groin with occasional radiation down the thigh to the knee.
Symptoms are usually exacerbated by physical activity and weight bearing and relieved by rest. In the late stages of osteonecrosis, pain is often present at rest, and patients may develop a limp, as they are no longer able to bear weight on the affected joint.
Osteonecrosis affecting the bone beneath a weight-bearing joint surface is associated with a significant risk of developing a subarticular fracture, which appears to initiate the symptoms.
Optimizing the dose of glucocorticoids has led to a significant reduction in the incidence of osteonecrosis post-transplantation. Substituting these agents entirely with calcineurin inhibitors may decrease this complication of the transplantation process even further. Early diagnosis using magnetic resonance imaging is essential for the success of available surgical interventions

Reference: https://www.sciencedirect.com/science/article/pii/B9780121835026500213
https://online.boneandjoint.org.uk/doi/full/10.1302/0301-620x.89b12.19400?journalCode=bjj&

Being an advocate for bone and joint pain and personally living with osteoarthritis osteonecrosis and spondylolisthesis pain .
I saw our community struggle in new and ways besides living and dealing with daily pain.
People suddenly couldn’t access routine care because of lockdowns, fear and added anxiety.
They became more isolated than ever before. They and their family members faced job losses and financial hardship.
As an advocate for arthritis and a facilitator for my local LIVE YES Connect Group, I had to cancel or postpone in-person programs and events.
But on the plus side we went virtual on Zoom
Some members and their families faced added strain, whether dealing with virtual school or safety concerns for loved ones in nursing homes.
It’s a year most are happy to see come to an end.
But as a person with pain, I am always compelled to find silver linings. Even in the mist of challenging of times.
In 2020, I got to travel to Washington D.C participate in a focus group and then speak on Capital Hill.
I met some fantastic people from our state representatives to other leaders and advocates who work so hard to create a strong support system for so many causes and conditions.
I got to stay in a great city and tour the beautiful historical city of Washington D.C
We made great strides in accessibility, as health care system finally embraced telehealth and more companies allowed remote work.
Many disabled now gave hope to possibly getting a part time job working from home now because we see it is doable.
We seen a President work tirelessly to get pharmaceutical companies to create a vaccine quickly that will be safe for the USA and world.
We gave witnessed the power of science and innovation with the development of promising treatments and vaccines.
We saw our neighbors and communities come together to support one another in their time of need.
Despite the news only showing negativity there was a lot of positive happening.
2020 shown how resilient we are. And to never lose faith. Be grateful for everyday.
I don’t know what 2021 will bring;
I’m hoping it will be a fantastic year.
I just want to Thank you for your support, and following me on IG, Blog, and all social media platforms I promise to bring you current and uplifting information in 2021 and I wish you all a safe, healthy, prosperous and happy new year

Several states have officially proclaimed today as Osteonecrosis awareness day this past year a few more states came on the awareness train. And by next year God willing all 50 state’s as well as the US Virgin Islands and Puerto Rico will as well.
I will post the entire list later
But for now – Below are some posts and info
https://avascularnecrosiseducation.com/2020/05/24/avascular-necrosis-mask/amp/
https://avascularnecrosiseducation.com/tag/educate/
Official Proclamation Avascular Necrosis-Osteonecrosis Awareness Day November 29
Question
Could you elaborate on how osteoarthritis can be a secondary condition to avascular necrosis? And how can avascular necrosis adversely affect a confirmed primary diagnosis of osteoarthriris?
That a great question and I will explain both with diagrams
Answer
Osteoarthritis and osteonecrosis (avascular necrosis) are two diferent problems. Osteoarthritis occurs with when the cartilage wears thin and degrades. It is thought to primarily a cartilage problem although recently some investigators have raised the theory that collapse of bone at the cartilage interface may also contribute.
Osteonecrosis occurs when the bone does not get enough blood supply and dies. This occurs most commonly after trauma to the joint injury, to say meniscus or a diver gets the bends . Patients with certain blood disorders, patients with lupus or those who are taking high doses of prednisone are also at risk for osteonecrosis.
The confusion comes when a joint is so badly degenerated or “at its endstage”.
So at that point it is often impossible to distinguish between the two problems.

There are many causes for developing Osteonecrosis aka Avascular Necrosis.
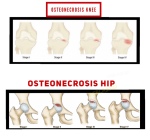
Osteonecrosis is a bone disease. It results from the loss of blood supply to the bone. Without blood, the bone tissue dies. This causes the bone to collapse. It may also cause the joints that surround the bone to collapse. If you have osteonecrosis, you may have pain or be limited in your physical activity.
Osteonecrosis can develop in any bone, most often in the:
It is also called:

Osteoarthritis is a joint disease that happens when the tissues in the joint break down over time. It is the most common type of arthritis and is more common in older people.
People with osteoarthritis usually have joint pain and, after rest, stiffness (inability to move easily) for a short period of time. The most commonly affected joints include the:
Osteoarthritis affects each person differently. For some people, osteoarthritis does not affect day-to-day activities. For others, it causes significant pain and disability.
#WEGOHealthChat #WEGOHealthAwards #PatientLeader #Osteoarthritis #Osteonecrosis #Grateful
ChronicallyGratefulDebla and https://avascularnecrosiseducation.com
Voting will begin in July and link will be posted then to vote.
Until then if you wish to nominate me or read about WEGOHealth please go to
WEGOHealthAwards Vote – Review Nominees – How It Works -The Judges
Many requested masks as so many cannot find them , so I contacted a local shop in my area and we made these two designs. The mask are washable
I don’t get paid anything for or a portion of the masks just doing this as a way to help those wearing a mask support the cause of Osteonecrosis aka Avascular Necrosis.
If you wish to purchase here is info. And they ship worldwide
They are closed on Sundays and Holidays

Afterburner FX
3600 Schotten Road
Hubbard Ohio 44425
3305347653 phone
Mask design
@Debla2020

